RCG Health TReatments
Summary
At RCG Health, we understand that effective weight loss is about restoring your health, improving quality of life, and reducing your risk of long-term illness.
We offer a full range of evidence-based metabolic treatments, including advanced medical therapies and weight loss surgery. Whether you’re exploring non-surgical options or considering an operation, our patient-centred programme provides expert care tailored to your needs, without requiring an NHS Tier 3 referral.
From your first consultation to long-term follow-up, we’re here to support you every step of the way.
Why Metabolic Health Matters
Metabolic health refers to how well your body regulates weight, blood sugar, blood pressure, and cholesterol. When these systems are out of balance, it can lead to serious health issues, including obesity, type 2 diabetes, fatty liver disease, and high blood pressure.
At RCG Health, we focus on treating the underlying drivers of metabolic dysfunction, helping you achieve sustainable weight loss and long-term health improvements.
What This Guide Covers
- Medical weight loss options, including new-generation medications and behavioural support
- The benefits and risks of both surgical and non-surgical weight loss treatments
- Surgical options: Sleeve Gastrectomy, Roux-en-Y Gastric Bypass, and One-Anastomosis (Mini) Gastric Bypass
- What to expect during recovery, including post-operative diet and activity advice
- Lifestyle guidance around pregnancy, alcohol, smoking, and mental wellbeing
- Ongoing care, including support for skin changes and long-term weight maintenance
Two Complementary Approaches — One Personalised Plan
We offer both metabolic medicine and metabolic surgery, which can be used independently or in combination:
Metabolic Medicine
A non-surgical pathway to weight loss and improved health, ideal for those not ready for surgery or who prefer a medical approach.
- Tailored dietary plans from registered dietitians
- Behavioural and psychological support to build lasting habits
- Access to effective, modern weight loss medications, including GLP-1 and GLP-1/GIP receptor agonists
- Close medical supervision and regular monitoring throughout treatment
Many patients lose 10–15% of their body weight through medical therapy alone, with some achieving even greater results.
These medications are generally well tolerated, but potential side effects may include nausea, vomiting, constipation, diarrhoea, abdominal discomfort, fatigue, and in rare cases, gallstones or pancreatitis. Most side effects are dose-related and tend to improve with time or dose adjustment.
For long-term success, ongoing treatment is usually necessary. Discontinuing the medication often leads to partial or full weight regain, especially if lifestyle changes are not well established. We work closely with patients to create sustainable strategies and discuss the benefits and risks of long-term use.
Metabolic Surgery
Surgery remains one of the most effective treatments for obesity and metabolic disease. Procedures reduce appetite, alter gut hormones, and improve conditions such as type 2 diabetes, high blood pressure, and sleep apnoea.
Our experienced team will guide you through your options and ensure you’re fully informed and prepared for each stage of the process.
When to Consider Each Option
Metabolic medicine and surgery are both powerful tools. Depending on your health goals and medical history, we may recommend:
- Medical therapy alone, as a first-line treatment or ongoing solution, especially for those with moderate obesity or who are hesitant about surgery
- Surgery, for those needing more significant or sustained results
- A combined approach, where GLP-1 medications are used as a preoperative measure to reduce surgical risk and improve patient outcomes
Supporting You for the Long Term
At RCG Health, we are committed to your long-term success. Whatever path you choose, our multidisciplinary team will help you stay on track with expert follow-up, emotional support, and practical guidance every step of the way.
Why Choose Bariatric Surgery?
Conventional weight loss methods, including diet, exercise, and pharmacological interventions such as GLP-1 receptor agonists (e.g., semaglutide [Ozempic, Wegovy], tirzepatide [Mounjaro]), typically achieve modest and often temporary results. GLP-1 medications may lead to an average total body weight loss of around 10–15%, with some individuals reaching up to 20% under ideal conditions. However, long-term adherence, tolerability, and weight maintenance after cessation of therapy remain significant challenges.
Endoscopic approaches, including intra-gastric balloons, typically result in a 7–15% of total body weight loss; however, the effects are often transient, and weight regain is common once the device is removed. These methods may be suitable for certain patients but do not typically lead to durable metabolic improvement in those with severe obesity or multiple comorbidities. In the very near future most will be replaced by
In contrast, bariatric surgery remains the most effective and durable treatment for clinically severe obesity. Surgical procedures, such as gastric bypass and sleeve gastrectomy, consistently result in 50–70% excess weight loss, equivalent to 25–35% total body weight loss, and offer proven long-term benefits.
Importantly, bariatric surgery is associated with high rates of remission or significant improvement in obesity-related conditions, including:
- Type 2 diabetes (remission rates of up to 80% in some patients)
- Hypertension
- Obstructive sleep apnoea
- Polycystic ovarian syndrome (PCOS)
- Joint pain and mobility limitations
- Sustained metabolic improvements
Large UK and international studies, including the Swedish Obese Subjects (SOS) study and NHS data from the National Bariatric Surgery Registry (NBSR), have demonstrated that bariatric surgery not only improves the quality of life and metabolic health but also reduces long-term cardiovascular risk and mortality.
While newer treatments, such as GLP-1 medications, are promising and may be part of a multidisciplinary approach, bariatric surgery remains the gold standard for individuals with a BMI ≥40 kg/m² or a BMI ≥35 kg/m² with significant obesity-related comorbidities, particularly when durable, life-changing outcomes are desired.
Which Weight Loss Surgery is Right for Me?
Choosing the most appropriate weight loss (bariatric) surgery depends on several personal factors, including your weight loss goals, medical history, eating behaviours, and any existing health conditions. Your surgical team will guide you through the decision, but the summary below provides a helpful starting point.
Understanding Your Options
Weight loss surgery, also known as bariatric or metabolic surgery, includes several well-established procedures. Each works slightly differently and offers distinct benefits. The main types performed at RCG Health are:
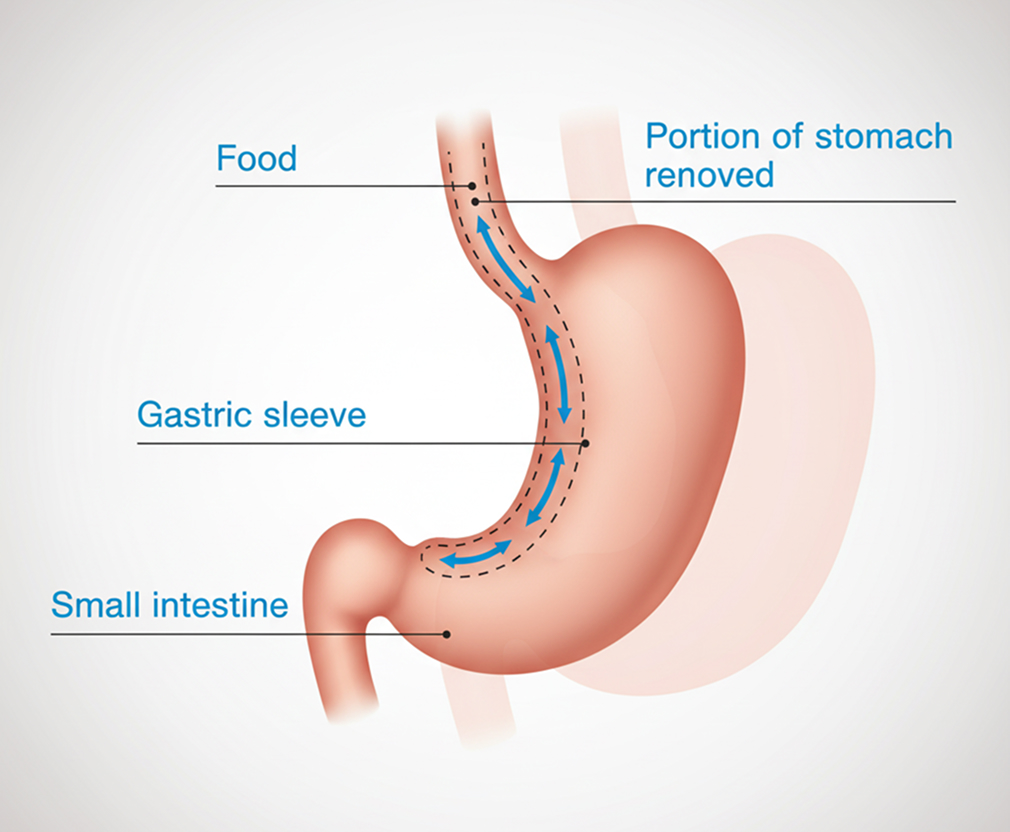
1. Sleeve Gastrectomy (SG)
- Removes around 75–80% of the stomach, leaving a narrow “sleeve”.
- Reduces hunger by removing the part of the stomach that produces the hunger hormone ghrelin.
- Does not involve bowel rerouting, so there’s less risk of nutritional deficiencies.
Best suited for: Patients without reflux or significant metabolic disease.
Expected results:
50–60% excess weight loss (EWL)
~25–30% total body weight loss (TBWL)
May worsen or cause new-onset reflux (GORD)
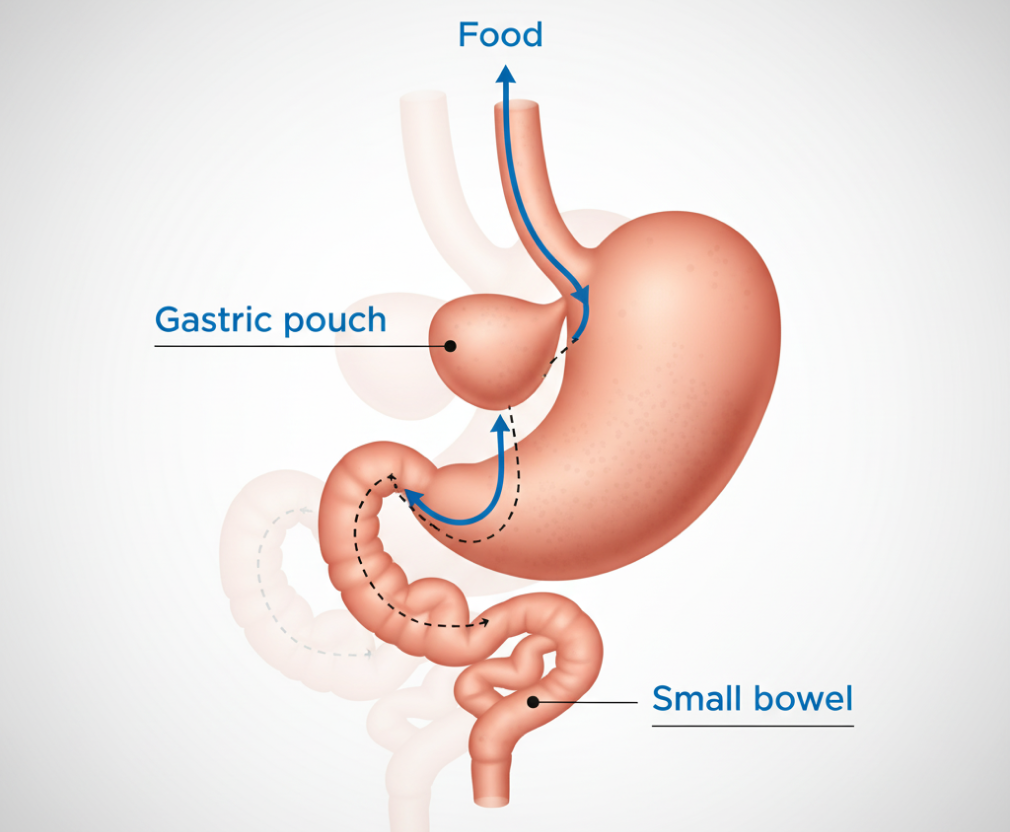
2. Roux-en-Y Gastric Bypass (RYGB)
- Creates a small stomach pouch and re-routes the small intestine to reduce both food intake and calorie absorption.
- Offers strong hormonal effects that improve blood sugar control.
Best suited for: Patients with type 2 diabetes or acid reflux.
Expected results:
60–70% EWL
~30–35% TBWL
Up to 80% diabetes remission in some patients
Requires lifelong vitamin and mineral supplements
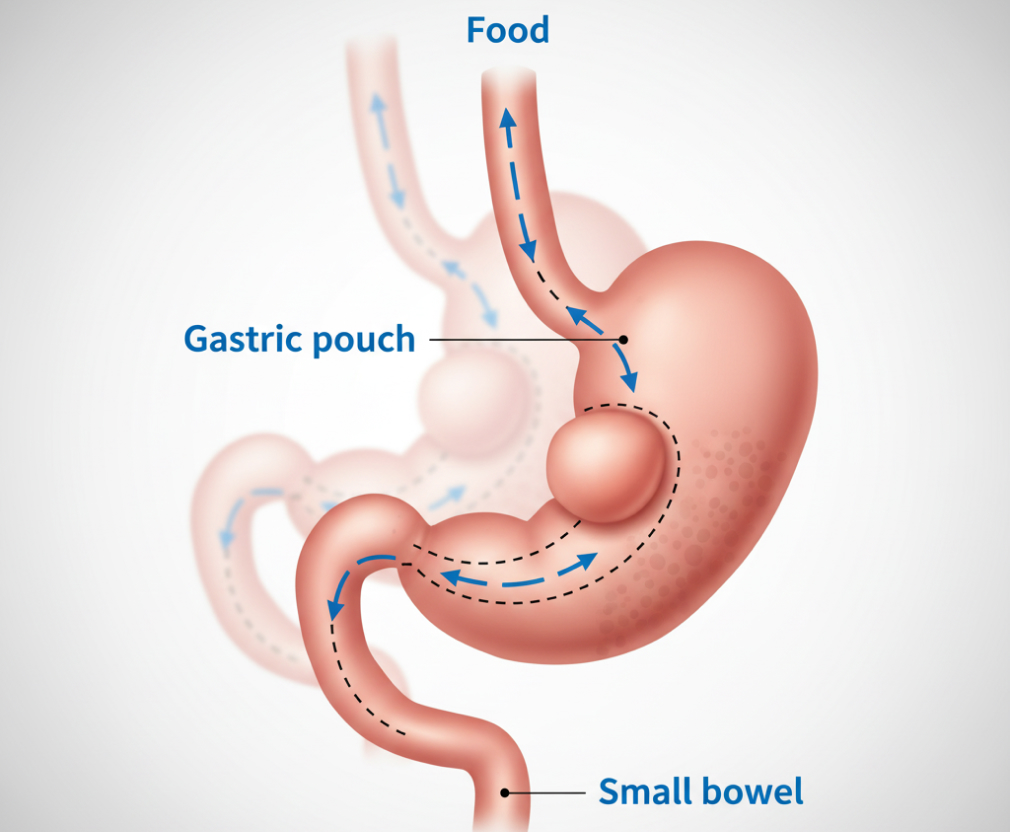
3. One Anastomosis Gastric Bypass (OAGB / Mini Gastric Bypass)
- A simplified bypass involving a single connection between the stomach and bowel.
- Offers similar weight loss and metabolic benefits to RYGB, with a shorter operation time.
Best suited for: Patients without bile reflux.
Expected results:
60–70% EWL
~30–35% TBWL
May cause bile reflux in a small number of patients
Key Considerations for Patients
How much weight will I lose?
- Most patients lose the bulk of their weight in the first 6–9 months.
- Weight typically stabilises between 12–18 months after surgery.
- Results vary by procedure and patient; long-term success depends on follow-up, nutrition, and lifestyle.
How will my diet change?
All procedures require permanent dietary changes:
- Smaller meals: You’ll feel full after less food.
- Protein-first eating: To preserve muscle during weight loss.
- Avoid high sugar/fat: Especially after bypass surgery, these can trigger dumping syndrome (nausea, sweating, cramps, diarrhoea).
- New food intolerances may arise — red meat, bread, and rice are common culprits.
What about reflux and diabetes?
- If you suffer from reflux, a gastric bypass may be a better option than sleeve gastrectomy.
- For those with type 2 diabetes or metabolic syndrome, bypass procedures often offer better long-term control and potential remission.
Do I need to take supplements?
Yes — all bariatric patients require lifelong vitamin and mineral supplements, with stricter regimens after bypass surgery due to reduced nutrient absorption.
Final Thoughts
There is no “one-size-fits-all” approach. Your surgical team will assess your goals, health status, and preferences to recommend the most suitable procedure. Whichever path you choose, the key to long-term success lies in your commitment to regular follow-up, healthy nutrition, and sustained lifestyle changes.
Benefits of Bariatric Surgery
Bariatric surgery is not cosmetic — it is a life-saving treatment with proven health benefits, including:
- Sustained long-term weight loss (typically 25–35% of total body weight)
- High remission rates of type 2 diabetes, particularly after bypass procedures
- Improved cardiovascular health, blood pressure, and cholesterol levels
- Enhanced mobility, joint health, and reduce chronic pain
- Improved fertility, especially in women with PCOS
- Better mental health, mood, and self-esteem
- Increased life expectancy and reduced risk of obesity-related conditions (e.g., heart disease, stroke, cancer)
These benefits are supported by large-scale studies, including the Swedish Obese Subjects (SOS) study and data from the UK’s National Bariatric Surgery Registry (NBSR).
Potential Risks and Considerations
While bariatric surgery is generally safe, all surgical procedures carry risks and require lifelong adjustments to diet and lifestyle. Important considerations include:
Surgical risks (though rare):
Bleeding, infection, blood clots, and leaks at surgical sites
Nutritional needs:
- Lifelong vitamin and mineral supplementation is essential after all procedures
- Bypass operations require closer monitoring due to reduced absorption of nutrients (e.g., vitamin B12, iron, calcium)
Digestive side effects:
- Nausea, vomiting, diarrhoea, and food intolerances may occur, especially in the early stages
Some patients experience dumping syndrome after bypass, especially when consuming sugary or fatty foods
Lifestyle changes:
- Alcohol should be avoided for at least 12 months post-surgery and consumed with caution thereafter
- Ongoing support from a multidisciplinary team (dietitian, psychologist, surgeon, GP) is key to long-term success
Bariatric surgery is a powerful tool — not a quick fix. When combined with a lifelong commitment to healthy eating, physical activity, and regular follow-up care, it offers a durable and effective solution for those living with severe obesity.
Your Bariatric Care Pathway
Embarking on a weight loss surgery journey requires careful planning and assessment to ensure you are fully prepared for the procedure and its postoperative care. Below is an outline of the process you will follow, from initial consultations to your pre-operative assessments.
Initial Workshop
To begin your journey, you can book an appointment (either in-person or virtual) with Mr. R. Camprodon. This session will cover:
- An overview of the various bariatric procedures, including their benefits and associated risks.
- Necessary dietary changes before and after surgery.
- A clear understanding of what to expect during your recovery.
- You will also undergo preliminary blood tests to help assess your suitability for surgery.
One-Stop Clinic
At this stage, you will attend a virtual One-Stop Clinic, where key members of your multidisciplinary team will assess you. Each expert will provide you with personalised care to ensure you are fully informed and supported:
- Surgeon: You will have a detailed discussion about the various procedures, their associated risks, and how each aligns with your goals and medical history.
- Metabolic Physician
- Nurse Specialist: This consultation will explore your personal preferences, surgical expectations, and any concerns you may have.
- Dietitian: To assess your current eating habits, nutritional needs, and readiness to make necessary lifestyle changes.
- Anaesthetist: A pre-operative assessment to evaluate your overall fitness for surgery, including any underlying health conditions that could impact anaesthesia.
Psychologist: Emotional readiness for surgery is crucial. The psychologist will help assess your mental and emotional well-being and offer additional support or therapy if required.
Multidisciplinary Team (MDT) Meeting
After your consultations, your case will be reviewed by the full bariatric multidisciplinary team (MDT). This collaborative meeting ensures that all aspects of your care are considered and the best next steps are determined. The MDT may recommend additional tests or provide a tailored care plan for your surgery and recovery.
Pre-Operative Assessment
Once you have been formally listed for surgery, you will attend a final pre-operative assessment to confirm your fitness for the procedure. This includes:
- Blood tests to detect any underlying conditions or nutritional deficiencies.
- Swabs to test for infections.
- Physical examination to assess your overall health and readiness for surgery.
This assessment ensures that any potential medical issues are identified and addressed before surgery, thereby reducing the risk of complications. Also includes recording your weight, height and BMI
Throughout your care pathway, you will be supported by our experienced team, ensuring you have the guidance and support needed to make informed decisions about your health and well-being.
The Pre-operative Liver Shrinkage Diet
Before undergoing bariatric surgery, you will be required to follow a liver shrinkage diet for 2 to 4 weeks (this comes separately from this leaflet). This is a crucial step in preparing your body for surgery and ensuring the procedure is as safe and effective as possible.
Why is this diet necessary?
- When you are overweight, the liver often becomes enlarged due to excess fat and glycogen (sugar) storage.
- An enlarged liver can obstruct the surgeon’s view and access to your stomach, making the operation technically difficult and potentially unsafe.
- The liver shrinkage diet is designed to reduce the size and weight of your liver by encouraging it to use up its stored glycogen and fat reserves.
- Following this diet significantly lowers the risk of surgical complications, such as bleeding or liver injury.
Why strict adherence is essential
- This diet is not optional — it is a critical part of your surgical preparation.
- If the liver remains enlarged, the surgeon may not be able to proceed safely. In some cases, the procedure may be cancelled or postponed on the day of surgery.
- Surgeons can tell during the operation whether the diet has been followed properly, so it is vital that you comply with the guidance given.
You will be expected to:
- Follow the specific diet plan provided by your bariatric team or dietitian, which may include meal replacement products (e.g., shakes, soups) or a low-calorie food-based alternative.
- Avoid high-fat and high-carbohydrate foods that contribute to liver fat storage.
- Drink plenty of fluids, as instructed.
- You will be expected to take Multivitamin supplements (A-Z complete) on this diet.
You will receive your personalised liver shrinkage diet plan from your dietitian, along with clear instructions and support. Please get in touch with us if you have any concerns or difficulties while following the plan.
Post-Operative Recovery
Your recovery journey is just as important as the operation itself. The early stages are designed to protect your healing stomach and help your body adjust to its new way of processing food.
Staged diet progression:
You will follow a structured post-operative diet in four key phases:
- Liquid diet – Week 1
- Puréed diet – Week 2
- Soft diet – Week 3
- Normal texture diet – From Week 4 onwards, with portion control and healthy choices
Physical activity:
Light walking is encouraged within days of surgery. Gradual return to normal activity over 4–6 weeks is typical, depending on the procedure and your recovery.
Follow-up schedule:
You will receive:
- Regular reviews with your dietitian, nurse specialist and surgeon at key intervals (e.g. 6 weeks, 3 months, 6 months, 12 months)
- Annual review up transitioned to your GP with clear monitoring guidance
Lifestyle Considerations
Successful long-term outcomes rely on lifestyle change as much as the surgery itself. Some key considerations include:
- Pregnancy: should be avoided for 12–18 months after surgery due to the risk of nutritional deficiencies during rapid weight loss. If you are planning a pregnancy, speak to your surgical team early for support and guidance.
- Smoking: must be stopped at least 6 months before surgery. Continuing to smoke increases the risk of anastomotic ulcers, poor healing, and complications. Long-term cessation is essential for your health and surgical success.
- Alcohol: should be avoided for at least 12 months post-surgery. Post-op, your tolerance may change, and alcohol is absorbed more rapidly, increasing the risk of liver damage and alcohol misuse. Pre-operatively, you should drink within UK Chief Medical Officers’ guidelines (no more than 14 units/week).
- Mental Health: while bariatric surgery is often associated with improved mood and self-esteem, it is not a treatment for pre-existing mental health conditions such as depression or anxiety. Emotional fluctuations post-surgery are common. Psychological support is available and encouraged, particularly during periods of adjustment.
Excess Skin After Weight Loss
Substantial and rapid weight loss may result in excess or loose skin, particularly around the abdomen, thighs, breasts, and upper arms. The degree of excess skin varies based on factors such as age, skin elasticity, starting BMI, and genetics.
Health implications:
Excess skin can lead to rashes, hygiene issues, and functional discomfort, particularly in skin folds.
Body contouring surgery (e.g. abdominoplasty or panniculectomy) may be considered to address this but:
- It is not routinely funded by the NHS and is subject to Individual Funding Requests (IFRs) based on medical need.
- In private practice, body contouring procedures are available but are not included as part of standard bariatric surgery packages.
Your surgical team can advise you on timing, candidacy, and realistic outcomes if this becomes a consideration in your long-term care.
Further Information and Support
For trusted advice, professional guidance, and patient support, we recommend the following resources:
British Obesity and Metabolic Surgery Society (BOMSS)
Up-to-date clinical information and patient resources from the UK’s professional body for bariatric surgery.
Obesity UK
A national charity offering peer-led support groups, advocacy, and resources for individuals living with obesity.
🔗 www.obesityuk.org.uk
Overview of Bariatric Procedures at a Glance
| Sleeve Gastrectomy | Roux-en-Y Gastric Bypass | One Anastomosis Gastric Bypass | |
|---|---|---|---|
| Operation Time | 1–1.5 hours | 2–4 hours | 1.5–3 hours |
| Hospital Stay | 1–2 nights | 1–2 nights | 1–2 nights |
| Surgical Method | Laparoscopic/keyhole | Laparoscopic/keyhole | Laparoscopic/keyhole |
| Nutritional Risk | Moderate | High: Potential deficiencies in iron, fat-soluble vitamins, calcium, and vitamin B12 typically | High: Potential deficiencies in iron, fat-soluble vitamins, calcium, and vitamin B12 typically |
| Potential Risks | GORD, bleeding, leaks | Dumping, ulcers, internal hernia | Dumping, bile reflux |
| Reversibility | Permanent | Rarely reversible | Potentially reversible |
| Weight Loss | 50–60% EWL | 60–70% EWL | 60–70% EWL |
| Mortality Risk | 0.2–0.4% | 0.2–0.4% | 0.2–0.4% |